
Children’s of Alabama, in collaboration with the University of Alabama at Birmingham Division of Transplantation, successfully performed a rare split-liver transplantation. This marks the first use of this lifesaving technique within the Children’s and UAB partnership in nearly a decade.
Split-liver transplantation, a highly complex procedure, allows a single deceased-donor liver to be divided and transplanted into two recipients located at separate hospitals. This innovative approach expands access to lifesaving organs, particularly for pediatric patients who depend on Children’s nationally recognized liver transplant program.

The transplant was led by UAB Assistant Professors of Surgery, Saulat Sheikh, M.B.B.S., and Marcos Pozo Jatem, M.D., working alongside Children’s of Alabama’s multidisciplinary transplant teams. The operation required a coordinated effort across both institutions, incorporating advanced machine perfusion technology to preserve the donor liver and extensive logistical planning for the out-of-state donor operation.
“This achievement represents the culmination of extensive preparation, education, and protocol development across multiple teams,” said Pozo Jatem, Surgical Director of the Pediatric Liver Transplant Program at Children’s of Alabama. “It involved close collaboration with the Pediatric Intensive Care Unit (PICU), hepatology, anesthesiology, pharmacy, nutrition, nephrology, and interventional radiology. It even resulted in the creation of a new intraoperative dialysis protocol to ensure this delicate procedure could be performed safely in critically ill patients.”
Pozo Jatem recognized the contributions of several Children’s and UAB team members whose expertise was essential to the effort, including Meloneysa Hubbard, MSN, CRNP, CCTC, who secured the use of machine normothermic perfusion; patient care coordinators Robin Greer, MSN, CPNP, and Julia Roberson, CRNP; and transplant surgery OR team leader Shannetta Simon, RN.
Additional key contributors from the partnership included David Willcutts, M.D., Assistant Professor of Pediatrics; Jeremy Loberger, M.D., Associate Professor in the PICU; and David Askenazi, M.D., MSPH, Professor of Nephrology.
“The availability of machine perfusion technology is a major advancement,” Pozo Jatem added. “It allows us to accept organs from across the country without increasing cold storage time, helping us maintain the highest possible viability of donated livers.”
According to Dr. Sheikh, who also serves as Surgical Director of UAB’s Living Donor Liver Transplant Program, “This successful split-liver transplantation is a significant milestone and an important step toward expanding access for many more patients on our waitlist. It reflects the extraordinary dedication of our jointly staffed teams at both Children’s of Alabama and UAB.”

In the early morning hours of Friday, May 31, 2024, around 30 maternal-fetal and neonatology experts filled an operating room at the University of Alabama at Birmingham Hospital. They were called in for an emergency cesarean delivery of quadruplets who were only 23 weeks and four days’ gestation.
As the babies were quickly delivered, the interdisciplinary team of physicians, nurses, and respiratory therapists jumped into action, fighting to keep the babies alive. Little did they know, they had delivered—and were going to save—the Guinness World Records title holders for the most premature quadruplets, breaking the record set back in 1997.

“When Lainey, Kali, Lennon, and Koen were born, they were 115 days premature,” said Becca Bryant, the quads’ mom. “A year later, we were surrounded by family and friends to celebrate their first birthday. It was a moment we were not sure we’d ever see.”
The Bryant quads made their entry into the world on May 31, 2024—Lainey at 2:15, Kali at 2:16, Lennon at 2:17, and Koen at 2:20 a.m. The neonatology team rushed them to the Level IV UAB Regional Newborn Intensive Care Unit, where they started UAB Golden Week protocols.
“The highest risk of complications and mortality for extremely preterm babies occurs during their first week of life,” said Colm Travers, M.D., neonatologist and director of the UAB Golden Week program. “The program focuses on minimizing complications in babies through that first critical week because it typically means a greater chance of survival and going home.”

Over the next five months, the quads received 24/7 care and monitoring. Becca rarely left their side, while Lavareis juggled work and taking care of the older kids, Kendall, Laikyn, and Kainen, and visits to Birmingham.
Little by little, the quads began to grow and improve. The numerous machines that kept them alive were slowly taken away as the quads’ own strength took over. In November, they were all stable enough to be transferred down to the UAB Continuing Care Nursery, a milestone for Regional Newborn Intensive Care Unit (RNICU) babies. Shortly after, the Bryants received news they were unsure they would ever hear—the babies were ready to go home.
Guinness World Record Holders
When Travers first met the Bryants, he discussed the risk, complications, and chances of survival for babies born at 23 weeks. He also realized he did not know of another instance where quads were born that early and all four babies survived.
As part of their delivery and care team, he and his colleagues in the UAB RNICU spent the next six months tirelessly working to help the babies survive and thrive. Travers, who is also an associate professor in the UAB Department of Pediatrics, secretly continued his research into the records of extremely premature babies.
Before the last baby was discharged, Travers had one more conversation with Becca and Lavareis.
“When my search came up empty, I realized there was a high chance the Bryant quads were the most premature quads to survive in the world,” Travers said. “Being able to tell them the exciting news, especially when our first conversation was not as optimistic, was a full-circle moment.”
The couple was, once again, in disbelief.
“Hearing our babies were the most premature quads put into perspective how lucky we were that all of them made it,” Becca said. “We had our family and friends, as well as the UAB team, there the whole way. Fighting for our babies, fighting for our family.”
More than a year after their birth, the quads had developed into happy 1-year-olds. All are now working with the PT/OT team on walking skills at Children’s and being followed for care. They also continue to visit the UAB Newborn Follow-Up Clinic.
For more information, click here.

Dallas, Marengo, Perry, and Wilcox counties, part of the Black Belt (so named for its rich, dark soil), are four of the poorest counties in Alabama. They also have one of the highest rates of childhood asthma—nearly 12% compared to the state’s 8%—and are severely underserved when it comes to medical care. Two of the counties don’t even have a pediatrician.
Yet just 4% of the more than 5,000 patients seen at Children’s of Alabama’s specialty asthma clinic hail from those areas. “We realized these kids weren’t getting to us for help,” pediatric pulmonologist Isabel L. Virella-Lowell, M.D., said. “But Medicaid data showed a high number of asthma-related claims from the area. So we knew there was a gap.”
One reason is distance, with families having to drive up to three hours to reach Birmingham. Thus, many children receive care only during asthma flare-ups at urgent care clinics or emergency rooms rather than ongoing, preventive treatment, said Children’s and University of Alabama at Birmingham (UAB) Pediatric Asthma Program Director Teresa G. Magruder, M.D. Without a primary care physician overseeing their child’s asthma, families find themselves caught in a cycle of crisis-driven care.
So instead of hoping kids will come to Birmingham, Virella-Lowell and Magruder are bringing their expertise to the Black Belt. Their mission: Improve those dismal asthma statistics by engaging the community at a grass-roots level.
The initiative began when Children’s and UAB infectious disease specialist Claudette Poole, M.D., spent time in the area studying water sanitation and parasites. She kept hearing about an asthma crisis and recruited Virella-Lowell and Magruder.
The three applied for and received a Health Resources and Services Administration (HRSA) grant, which provides salary support for the core team along with local community and health care partners. It also helps fund the virtual continuing medical education (CME) Project ECHO sessions, health fairs, and supplies such as spirometers and educational materials.
Magruder and Virella-Lowell stress the community-based approach of their efforts rather than having Children’s swoop in for just a few months. “We are really trying to improve the capacity of the community and their understanding of delivering asthma care in their own communities,” Magruder said. That means educating the frontline people caring for children, including school nurses, teachers, daycare workers, and parents, while providing access to subspecialty care for the severe high-risk patients.
“Our goal is to raise the level of asthma care across the state,” Magruder said, “not just at Children’s, but everywhere kids need it.”
To see the full story, click here.

Successfully stemming rising rates of cardiovascular disease in adults needs to start in childhood. But with mounting numbers of children and adolescents developing high blood pressure—a trend driven largely by skyrocketing obesity rates—this objective is getting harder to achieve. Enter the Pediatric Hypertension Program at Children’s of Alabama, which, with its steady growth, seeks to break the cycle.
The Hypertension Clinic, which operates three half-days each week, now sees about 45 patients weekly, a tenfold increase from 14 years ago, says Daniel Feig, M.D., Ph.D., director of the Division of Pediatric Nephrology at Children’s, who was recruited in 2011 to oversee the clinic’s development and expansion.
Drawing patients from across Alabama as well as some from eastern Mississippi and western Georgia, the Children’s Hypertension Clinic provides ongoing care for about 2,200 children. But this catchment area is likely home to about 70,000 young people with high blood pressure who are undiagnosed. Part of the problem is that many pediatricians aren’t comfortable diagnosing or treating the condition, Feig explains.

When patients come to Children’s, they’re often set up with ambulatory blood pressure monitoring equipment they wear for 24 to 48 hours to measure blood pressure a few times each hour while doing normal activities. The technology enables Children’s clinicians to tease out who actually has hypertension and not blood pressure spikes resulting from factors such as exertion, nervousness, or pain.
Once diagnosed, Feig and pediatric nurse practitioner Jessica Edmondson collaborate with dietitians, pharmacists, social workers, and others at Children’s to ensure patients benefit from a multidisciplinary approach to treatment. Ultimately, they’re trying to prevent both short- and long-term health implications resulting from hypertension, including heart thickening, retinal damage, and even impairments in cognitive function.
It’s a daunting task, Feig acknowledges. “Anything we can do to reduce the numbers right now has a domino effect that reduces long-term target organ damage and long-term cardiovascular risk,” he said. “We’re not at a point where we can reverse the trajectory in 70,000 undiagnosed kids in Alabama, but we can positively impact a good number of kids, improve their health and quality of life, and gain the opportunity to gradually access more and more of them.”
To see the full story, click here.

As the reputation of the Children’s of Alabama Pediatric and Congenital Heart Center of Alabama has grown, so has the success of its programs. Case in point—Hearts at Home, an interstage home monitoring program for any patient with single ventricle physiology who has undergone their first palliation procedure. In the last five years, the program has seen steady growth in the number of these patients, and leaders say the center’s reputation is among the reasons why.
“I think as a heart center in general, we've just had an influx of patients,” said Brittney Abercrombie, a nurse practitioner and the coordinator of Hearts at Home. “And so by default, that means that we are having more interstage patients.”
When Abercrombie moved into her role five years ago, Hearts at Home was caring for six to eight patients at a time. Now, she says they typically have about 13. Yearly, the program follows as many as 30, compared with 23–25 when she began. In the last couple of years, they’ve attracted more patients from outside Alabama, including children from Georgia, Tennessee, and the Pensacola, Florida, area. Some of the program’s patients chose Children’s over other options in the region.
“I think they recognize that our outcomes here are some of the best in the Southeast,” said Alan Brock, M.D., the program’s medical coordinator. “And when they have the opportunity to look around and pick which program they want, I think patients are choosing us.”
As a result of the program’s success, hypoplastic left heart syndrome—a condition that brings many patients to the program—has become one of the most common forms of single ventricle congenital heart disease the hospital treats, Brock added. “I think it's because we’re getting better at what we do, and we’re saving a lot more lives now,” he said. “That is part of the reason that there are more patients coming into our program.”
For a closer look at the program and the difference it is making, click here.
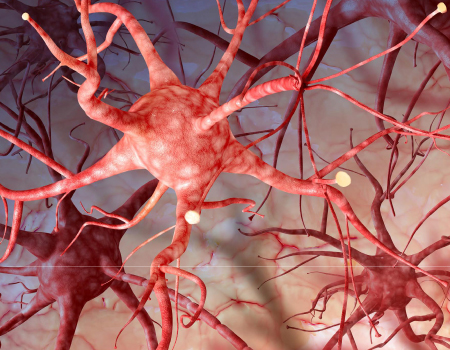
Neurofibromatosis (NF) is a complex genetic disorder of the nervous system, marked by the growth of tumors—malignant and benign—along nerve sheath cells. In addition to tumor growth, it impacts nearly every organ, including the skin, eyes, heart, and bones, and causes neurological symptoms such as ADHD, speech disorders, and learning disabilities.
There is no cure, although new treatments are emerging. Thus, it requires intensive management with a multidisciplinary team, which is exactly what the Neurofibromatosis and Schwannomatosis Clinic at Children’s of Alabama and the University of Alabama at Birmingham (UAB) is designed to do.
Neuro-oncologist Rebecca Brown, M.D., Ph.D., directs the adult portion of the clinic, and pediatric neuro-oncologist Katie Metrock, M.D., directs the pediatric side. The two work closely together, with Brown seeing patients as young as 12 and both teaming up to create a transitional program for children moving into adult care.
“The disease affects every aspect of these patients’ lives,” said Brown, who moved to UAB from Mount Sinai Health System in New York City. “I tell people that I’m the most generalist sub-specialist that exists because NF experts are the only ones who really understand, pay attention to, and address all these many aspects.”
“Even though they all have the same diagnosis of NF, every patient is different, and every family is a little different,” Metrock said. “So how do we approach care in a way that makes the most sense for each patient?”
For Brown, that means shifting the adult clinic from one that’s been focused on diagnosis, genetics, and disease phenotype to one that can have a greater clinical impact on patients. “My focus is patient-forward,” she said. “I’m interested in addressing the problems that patients experience, especially with regard to supportive care—including psychological care and pain management—and delivering the most recent recommendations for tumor surveillance and other health risk factors such as hypercholesterolemia, stroke, and heart disease.” She also wants to bring more clinical trials to UAB to “try to push the envelope as far as developing novel therapies for their conditions.”
On the pediatric side, non-medical specialists such as social workers, child life specialists, and school liaisons provide the holistic level of support children and their families require. “There’s so much that needs to be to be managed outside of our clinic with these children,” Metrock said. “So the social worker and school liaison really help bridge the gaps between school and life.” The clinic also works closely with the Hope and Cope team to help address neurocognitive and mental health issues.
“We’re very committed to providing care for these patients, not just for their tumors, but for how the disease affects their life outside of our clinic,” she said.
For an in-depth look at the work Brown and Metrock do, click here.
The Because We Care Questionnaire initiative rolled out across the hospital for inpatients and clinic visits via MyChart, MyChart Bedside, or eCheck-in For All. This technology allows patient families to self-report needs and barriers to care they are facing. Notifications are sent to the social work team when needs are reported, which allows social workers to follow up with families and provide resources to address barriers related to food insecurity, transportation needs, and housing instability.
Because of this initiative, we are more proactively addressing barriers to care for the families we serve.
Sepsis is a life-threatening condition when the body’s response to any type of infection spirals out of control and triggers widespread inflammation that can lead to tissue damage, organ failure, and even death if not addressed quickly. Every year, more than 75,000 U.S. children get severe sepsis, and 6,800 children die from sepsis. Survivors can be left with long-term disabilities.
Children’s of Alabama is preventing these tragedies through a relentless focus on quality improvement, standardized care bundles, and robust patient-safety programs. By embedding evidence-based interventions into clinical practice, mortality can be curtailed, hospital stays shortened, and ICU utilization can be reduced.
From 2016 to 2023, Children’s participated in the Improving Pediatric Sepsis Outcomes (IPSO) collaborative uniting 66 children’s hospitals, tracking more than 100,000 pediatric sepsis episodes to drive data-informed change. Through multimodal QI methods and a lifesaving care bundle, IPSO members achieved:
The Sepsis Committee has optimized the EHR to work faster and smarter through:
Sepsis cannot be discussed at Children’s without acknowledging the efforts of the Emergency Department. They have been a leader in the recognition and care of children with sepsis and have consistently maintained their times to fluid boluses and antibiotics under the treatment goals.
In alignment with the Solutions for Patient Safety (SPS) Safety Disparities Foundations Roadmap, the Health Disparities Improvement Team (HDIT) at Children’s of Alabama has made substantial progress in addressing race and ethnicity (R&E) data collection, identifying disparities, and laying the groundwork for meaningful interventions. This work is essential to reducing harm and ensuring the best pediatric care outcomes, regardless of demographics.
The SPS Safety Disparities Roadmap includes six key stages. In 2025, Children’s made progress up to the fourth.
Part 1: Establishing Foundations for Safety Disparities Work (Completed)
Part 2: Examining Race & Ethnicity Data Collection Processes (Completed—Moving to Green Zone)
Part 3: Building a Reliable Safety Disparities Data Set (In Progress)
Part 4: Analytical Foundations—Understanding Safety Disparities Data (Early Stages)
By systematically following the SPS road map, Children’s is building a strong data-driven approach to eliminating pediatric healthcare disparities. HDIT remains committed to ensuring safety and high-quality care for all children.

In 2025, Children’s of Alabama welcomed a new medical dog, Sydney. She is a golden retriever and the second dog to join the Child Life and Education team. She works alongside her child life specialist handlers to provide support to patients and families receiving care for cancer or blood disorders in the hematology/oncology department.